Royal Dental College
E-ISSN: Coming Soon
E-ISSN: Coming Soon
Beyond the obvious: Case report of an innocuous tongue lesion concealing a Neurilemmoma
Full Html
INTRODUCTION
Schwann cells surrounding peripheral nerve fibers are the source of benign tumors known as Neurilemmomas.[1] The growth of Schwann cells in the epineurium is thought to be the cause of the lesion, which displaces and compresses the nearby normal nerve. It typically develops in conjunction with a nerve trunk and is a well-encapsulated, asymptomatic slow-growing tumor.[2] It is uncertain what causes Neurilemmoma. Numerous etiological factors have been found, including spontaneous growth, external damage, persistent pain, and radiation exposure.[3] The spinal, cervical, sympathetic, vagus, peroneal, or ulnar nerves are typically the source of it. Only 1% of all schwannomas have an intraoral origin, while 25% are extra cranially found in the head and neck. It exhibits a preference for tongue intraorally. Schwannomas can develop at any age; however, their most common occurrence ranges from third to sixth decades.[4] In this article we describe a case of tongue Neurilemmoma in a 22year old female patient along with histopathological analysis and discussion of the differential diagnosis.
CASE REPORT
A 22-year-old female patient presented with a growth on the dorsal aspect of her tongue that had been present for one year. (Fig 1). There was no accompanying pain or tenderness noted. On intraoral examination, a well-defined mass of approximately1.0 x 0.8 cm diameter was found on the dorsal surface of the tongue on the center aspect. The lesion was sessile and nodular. The color of the overlaying mucosa was normal. A provisional diagnosis of fibroma was made. The lesion was completely surgically excised under local anesthesia. Tissue specimen was sent for histopathological examination.
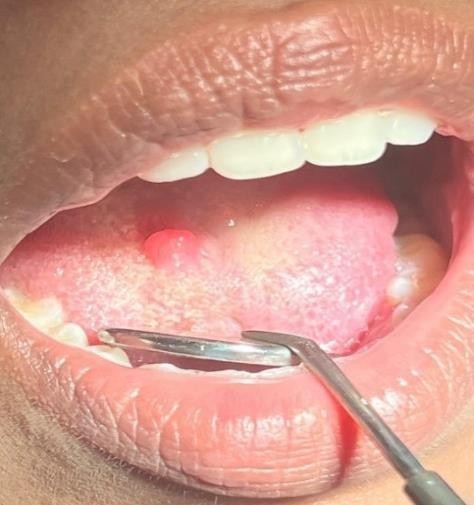
Fig 1: A nodular growth on the dorsal surface of the tongue
On gross examination, the specimen was well-encapsulated, firm, cream white in color measuring 0.8 x 0.5cm in diameter (Fig 2). The H&E stained tissue section showed a well-circumscribed connective tissue lesion consisting of hyper cellular areas with spindle shaped cells having elongated wavy nuclei (Antoni type A). Homogenous eosinophilic acellular areas with peripheral nuclear palisading of nuclei resembling Verocay bodies (Fig 3A & B) were present. A few hypo cellular areas in a myxomatous stroma (Antoni type B) and numerous small and medium sized endothelial lined blood vessels were also observed. The overlying epithelium was atrophic. Histopathology was confirmative with Neurilemmoma.

Fig 2: Gross specimen surgically excised from the dorsal surface of the tongue
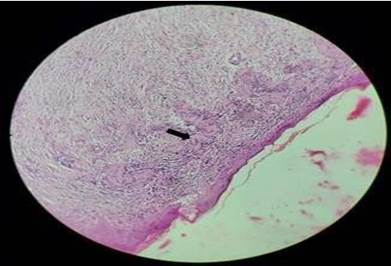
Fig 3A: Photomicrograph of the lesion showing Antoni type cells (H&E; 100x)
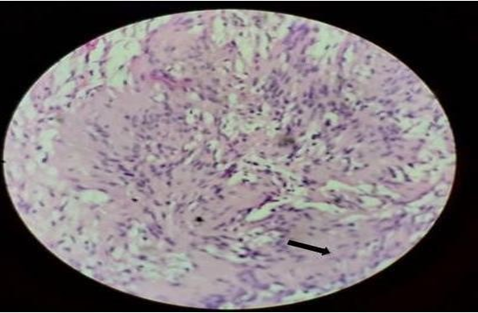
Fig 3B: Showing Verocay bodies in Schwannoma (H&E; 400x)
DISCUSSION
The Schwann cells of any peripheral autonomic or cranial nerve, with the exception of the Olfactory and Optic nerves, are the source of Neurilemmoma, also referred to as Schwannoma or Neurinoma of "Verocay".[2] Verocay was the first to describe them in 1908.[4] They often manifest as single lesions, though syndromes may be linked to several lesions.[2] 5% have meningiomatosis with or without NF2, 2% have Schwannomatosis, 3% have Neurofibromatosis type 2 (NF2), and about 90% are sporadic.[5] Only 1% of instances have an intraoral origin, with the majority (between 25 and 48%) occurring in the head and neck area. The most frequent intraoral location is the tongue, which is followed by the palate, gingiva, lip, buccal mucosa, and floor of the mouth.[2] It is challenging to determine from which nerve it started in our patient. Nonetheless, this mass may originate from Schwann cells surrounding the glossopharyngeal, Vagus, or Hypoglossal nerves.[1] Gender preference is not evident in the majority of investigations. Schwannoma is the most prevalent peripheral nerve tumor in adults, while it can occur in children of any age with an incidence of 0.3 to 0.4 cases per 100,000 people annually.They are most common in those aged 30 to 60.[6] Tongue Schwannoma is most frequently observed in second to fourth decades of life.[1] They are usually benign neoplasms that grow slowly and show no symptoms. When they enlarge and press against the affected nerve, they could exhibit minor pain.[2] Our patient belonged to same age group typically affected by sporadic tongue Schwannoma and did not report any pain in the mouth. Schwannomas are rare and typically excluded from the differential diagnosis of intraoral soft tissue tumors. Less than 50 cases of lingual Schwannomas have been documented in the literature over the past 20 years, despite the fact that the tongue is the most often occurring intraoral tumor site for Schwannoma. This could indicate that some cases are being underreported or ignored. Since Schwannomas are clinically identical to other benign soft tissue tumors, they could be difficult to diagnose. These consist of leiomyoma, lipoma, fibroma, neurofibroma, traumatic neuroma etc. Neurofibromas can occur deeper within the body, close to nerve plexuses (plexiform neurofibroma) or on the skin (cutaneous neurofibroma). The most prevalent manifestation of NF1 is neurofibromas, which are benign tumors made up of nerves, mast cells, macrophages and fibroblasts.[7] A traumatic neuroma is a non-neoplastic growth of neural tissue that develops after surgery or an injury. In a clinical setting, it manifests as a nodule that is occasionally tender on palpation. The lip, tongue, and mental nerve area are the most often occurring oral sites.[8] An oral fibroma is regarded as a benign fibrous tissue growth that develops in response to irritation or trauma. It usually has a hue that matches the surrounding tissue and is hard, nodular, and painless. It can be found in sites including the lip, tongue, and buccal mucosa.[9] Mature white adipose tissue makes up lipomas. They range in color from yellow to orange and are highly isolated from their surroundings.[10] Oral leiomyomas are uncommon, manifest in a broad age range and begin in the fourth to sixth decades of life. Most of the oral leiomyomas are solid or vascular in morphology.[11] Therefore, a confirmative diagnosis requires a biopsy and histopathological analysis. The diagnosis is also aided by imaging procedures like MRI and USG.[6] Schwannomas are characterized by a biphasic pattern of alternating myxoid hypocellular Antoni B areas and hypercellular Antoni A spindle cell areas. Verocay bodies are created by nuclear palisading around fibrillary processes. Rarely, we can see hemorrhage, necrosis, and mitotic activity.[12] These features were also present in our case. Schwannoma tumor cells are encased in a pericellular basal lamina that contains collagen type 4 and laminin, and they exhibit consistent, high nuclear and cytoplasmic S100 immunoreactivity. Antibodies to glial fibrillary acidic protein (GFAP) may also cause Schwannomas to exhibit immunoreactive and some of these tumors also express cytokeratin.[13] Complete surgical excision is the preferred course of treatment for a single lesion and the likelihood of recurrence or malignant change is quite low (8–10%).[2] An excisional biopsy was performed in this case because the lesion was small and clearly defined and the patient did not exhibit any signs of nerve damage after the procedure.
CONCLUSION
There are extremely few occurrences of tongue Schwannoma documented in the literature and it is rare particularly in younger age groups. Tongue Neurilemmomas may be underreported in medical literature since they are not commonly encountered by health care practitioners. Due to its clinical similarity with other soft tissue tumors of the oral cavity, including fibroma, neurofibroma, benign salivary gland tumors, leiomyoma, rhabdomyoma, lymphangioma, and hemangioma, it demands careful clinical and histopathologic examination. A histopathologic assessment is necessary for the final diagnosis. Complete surgical removal of the lesion is the course of treatment. There is barely any chance that the lesion will recur or become malignant.
References
